Health Concerns
Anxiety and Depression
ADHD
Autoimmune Disease
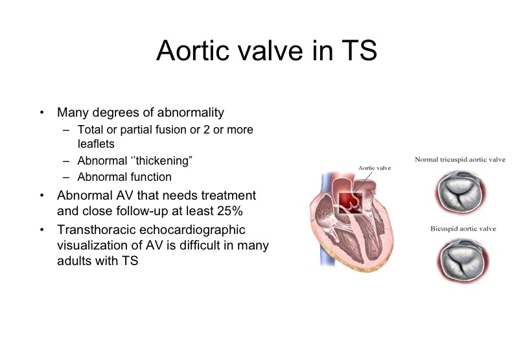
Cardiovascular Disease
Celiac Disease & Gastrointerology Issues
Dental & Oral Care
Developmental Delays
Diabetes
Ears & Hearing
Eyes
Growth
Hypertension
Liver
Lymphatic System
Renal Function
Sexual Development
Skeleton & Bones
Skin & Nails
Therapeutic Interventions
Thyroid

Females with TS have an increased prevalence of auto-antibodies and are at increased risk of developing autoimmune diseases compared to the general population. The absence of a normal second X-chromosome further contributes to increased autoimmunity in TS. Health care providers should be observant and test liberally for these conditions even before clinical symptoms emerge.
Autoimmune diseases include:
Hashimoto thyroiditis, pernicious anemia, Addison disease, celiac disease, inflammatory bowel disease, diabetes, autoimmune hepatitis, autoimmune colitis, thrombocytopenia, and juvenile rheumatoid arthritis
Celiac Disease Symptoms:
Classic Symptoms
- Anorexia
- Diarrhea
- Bloating/gas
- Vomiting
- Constipation
- Lactose intolerance
- Abdominal pain
- Pale or foul smelling stool
- Weight loss/muscle wasting
Non-classic symptoms
- Failure to thrive infants
- Anemia resistant to oral iron therapy
- Autoimmune thyroid disease
- Unexplained short stature or delayed puberty
- Depression, irritability, learning or behavior disorders
- Seizures
- Neropathy/ataxia
- Recurrent fetal loss (intrauterine growth retardation)
- Delayed or missed periods/infertility
- Osteoporosis/osteopenia
- Oral sores
- Loss of tooth enamel
- Vitamin deficiencies
Diagnosis of Celiac Disease:
Serology
- Total Serum IgA
- Tissue transglutaminase antibody (tTg-IgA) (tTg-IgG if IgA deficient)
- AGA IgA if less than 5 years old
Small bowel biopsy
- Villous atrophy
- Crypt hyperplasia
What is Gluten?
Gluten is the trigger for the inflammatory response of celiac disease.
Gluten is a general name for storage proteins. Sorage proteins in wheat, barley, and rye are harmful to celiacs. These grains and any ingredient that comes from them are eliminated in a gluten free diet, including spelt, kamut and triticale.
More resources for Celiac Disease
Celiac Presentation Materials
A Color Handbook of Pediatric Gastroenterology; Pohl, Jolley, Gelfond 2014
back to top

Since Turner syndrome was first described in 1938, pediatric endocrinologists, cardiologists and other specialists have done extensive research to better understand the disorder and improve quality of life for patients. Many advancements in the treatment of the disease have been made; at present, for example, growth hormone therapy can increase final adult height in women with Turner syndrome...Read more

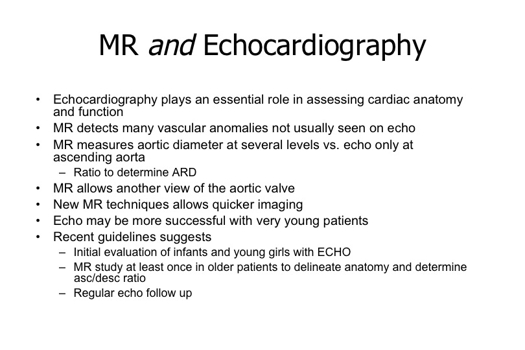
MRI - According to Paul H. Saenger, the sensitivity of MRI in the detection of cardiovascular problems in patients with Turner syndrome is superior to echocardiography. “Therefore,” Saenger said, “an MRI is the method of choice for all patients past the age of 10 years.”
Endocrine Today news article
The Heart in Turner Syndrome pdf
Leo Lopez MD
Director of Pediatric Cardiac Noninvasive Imaging
Children’s Hospital at Montefiore
Associate Professor of Clinical Pediatrics
Albert Einstein College of Medicine
Have more questions? View our FAQs about Cardiovascular Disease in TS
back to top

Dental Health Considerations & Solutions in Patients with Turner Syndrome
Robert Korwin, D.M.D.
Post Graduate Certificate in General Practice
Master, Academy of General Dentistry
Master, International College of Oral Implantologists
Member, Board of Directors, American Society for the Advancement of Anesthesia in Dentistry New Jersey Sedation Permit
Graduate, Progressive Orthodontic Seminars
White Paper
Oral Manifestations of Turner Syndrome
Kimberly Ann Bailey Walker, RDH, BS, BSN
August 2014 Course - Expires August 31st, 2017
American Dental Hygienists' Association
CDE Activity
Early steps to good oral health in your child:
- Clean your child’s mouth twice a day even if he/she does not have teeth yet. Wipe his/her gums with gauze. Anything that touches someone else’s mouth should not be allowed to touch his/her mouth.
- Once the first tooth appears, use a soft-bristled toothbrush and water to brush your child’s teeth.
- Children should have their first dental visit around the time of their first tooth eruption and no later than age 1.
- There should be 20 teeth in your child’s mouth by age 3.
- Never put your child to sleep with a bottle containing anything but water.
- Routine exams should occur every six months or as determined by your child’s dentist.
- Once your child learns not to swallow toothpaste, brush his/her teeth with a rice-sized speck of fluoride toothpaste.
Dental Issues In Turner Syndrome, Children's Hospital at Montefiore, Aug. 2013
Dr. Farrah Alam, DDS
Director, Special Care Dentistry
Rose F. Kennedy Center
Albert Einstein College of Medicine
slide presentation
back to top


Cognitive and Academic Performance
No increase in the prevalence of mental retardation is associated with TS, except for those few patients with a small ring X chromosome that fails to undergo X inactivation. Numerous studies have documented, however, that some individuals with TS have selective impairment in nonverbal, visual-spatial processing and as a group score lower on the performance than on the verbal subsection of standardized intelligence tests. Read more about Learning.
Sexual Development
Sexual infantilism is one of the most common clinical findings in girls with TS. Over 90% have gonadal failure. It is important to remember, however, that up to 30% of girls with TS will undergo spontaneous pubertal development, and 2–5% will have spontaneous menses and may have the potential to achieve pregnancy without medical intervention. Pubertal development may be delayed and, in most patients, is followed by progressive ovarian failure and Reproductive Health.
Social Issues
Adjustment problems in the areas of immaturity, difficulties in the ability to concentrate, and increased activity levels have been documented in young girls with TS. For adolescent girls, immaturity and anxiety appear to be the central issues. Girls with TS have been found to have more problems in school and with peer relationships than short girls without TS. Read more on Emotional Impact.
back to top

Glucose Intolerance
Glucose intolerance occurs more frequently in persons with Turner syndrome than in the general population; however, diabetes mellitus seems to be rare. Monitoring of fasting blood glucose concentrations should be considered in girls who are significantly overweight, have a strong family history of type 2 diabetes mellitus, are Hispanic or African American, or have signs of insulin resistance, such as acanthosis nigricans.
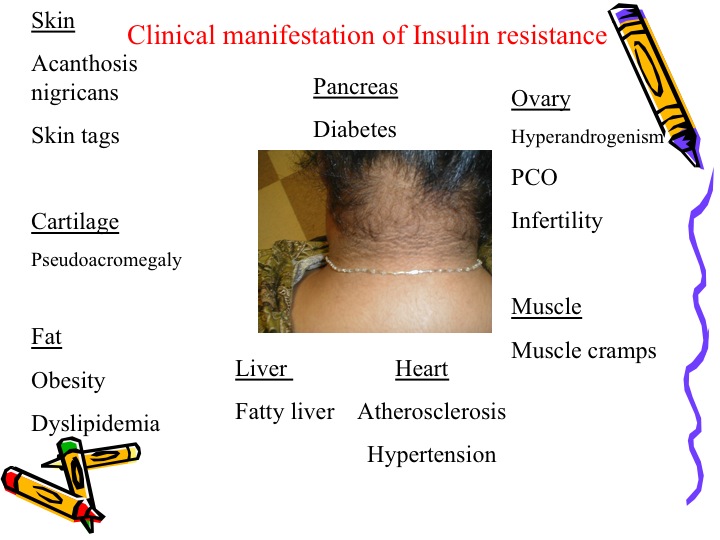
Obesity
Obesity is a problem in Turner syndrome. Diet and exercise for weight control should be part of a healthy lifestyle. Women with Turner are at a moderately increased risk of developing type I diabetes in childhood and a substantially increased risk of developing type II diabetes by adult years. The risk of developing type II diabetes can be substantially reduced by maintaining a normal weight. The reason for the high risk for diabetes amongst individuals with Turner is unknown. Type II diabetes can be controlled through careful monitoring of blood-sugar levels, diet, exercise, regular doctor visits and sometimes medication. The incidence is not increased by treatment with growth hormone.
Healthy women with Turner syndrome are characterized by:
- Impaired glucose tolerance
- Insulin resistance
- Low physical capacity
- Enlarged type IIa muscle fibers, indicating diminished oxygen and substrate supply for metabolic processes.
- These findings could be indicative of a prediabetic state.
Maintaining a Healthy Weight
- Self-monitoring: Be aware of the certain risks associated with obesity.
- Stimulus control: Creating stimulus control to increase awareness, physical activity, healthy food choices and an optimistic outlook.
- Contingency management: goal setting, reinforcement, and contracting
- Modeling and social skills
- Cognitive skills: reframing, self-efficacy, problem solving, relapse prevention
- Focus on health rather than appearance
- Encourage preference for healthful foods, awareness of hunger and satiety
- Emphasize physical activity
- Teach behavior change techniques
- Use social support
- Improve parent-child interaction
back to top

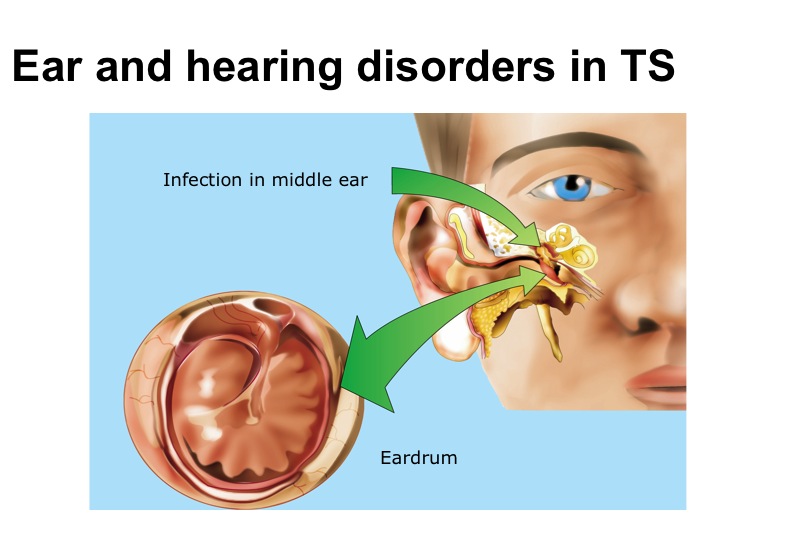
Hearing
Conductive and sensorineural hearing loss are common in girls with TS. The outer, middle, and inner ear are all affected, and hearing problems and ear malformations correlate with the karyotype.
How We Hear 101
The ear is divided into 3 parts that lead up to the brain.
The External Ear: sound travels down the ear canal and strikes the ear drum causing it to vibrate.
The Middle Ear: Vibrations from the ear drum cause the ossicles to vibrate which then creates movement of the fluid in the inner ear.
The Inner Ear: the movement of the fluid in the inner ear cause changes in tiny hair cells. Movement of hair cells sends electrical signals from the inner ear to the auditory nerve which leads to the brain.The brain then interprets these electrical signals as sounds.
Degree and Types of Hearing Loss
Hearing loss is described in terms of degree of severity:
Normal:
0-15dB for children
0-25dB for adults
Conductive Hearing Loss:
Problems within the outer and/or middle ear
Bone conduction hearing is within the normal range
Air conduction hearing can range from mild to moderate-severe
Ear infections and otitis media (fluid in the middle ear) are common in childhood because of the position of the Eustachian Tube early in life.
Children with TS are at even greater risk for middle ear problems and are thought to be pre-disposed to middle ear problems due to ear malformations and abnormalities. Some persistent middle ear problems can lead to sequelae such as TM perforations, drainage and the development of cholesteatomas.
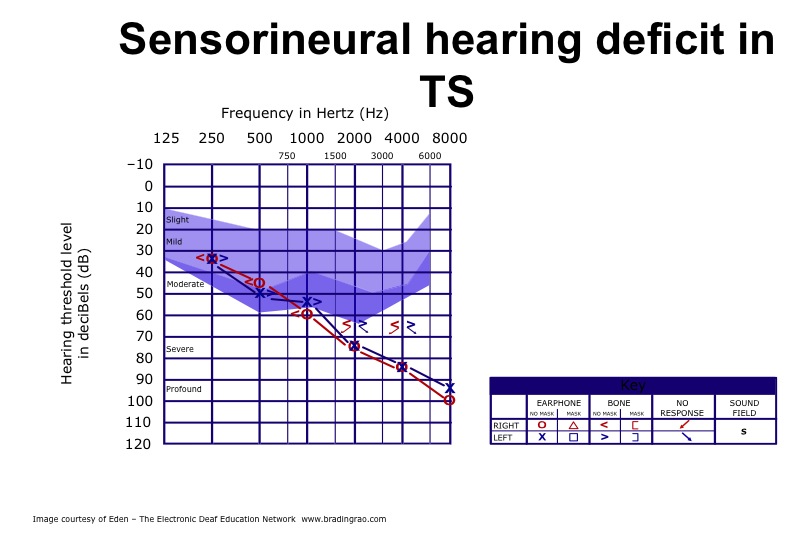
Sensorineural Hearing Loss:
There are problems within the inner ear. Bone conduction and air conduction are approximately equal and can range from mild to profound. Studies shows there can be either a progressive SNHL with a midrange bilateral symmetric dip in the 1.5-2.0kHz region or a high frequency downward sloping SNHL. Most common onset for a patient with TS is during the 2nd and 3rd decades of life but may be present as early as 6 years old. This hearing loss may begin in childhood and worsen over time, more than 90% of women with TS in their forties have some degree of HL and more than 25% of them need hearing aids.
Mixed Hearing Loss:
Problems within the outer and/or middle ear as well as inner ear.
Hearing loss by both bone conduction and air conduction.
Hearing loss via air conduction is greater than hearing loss via bone conduction.
Tympanometry
Assessment of the function of the ear drum (tympanic membrane)
Classification:
Type A – WNL
Type B – Flat (fluid, cerumen, TM perf)
Type C – Retracted/negative pressure
Type Ad – Hypermobile
Type As – Stiffness
Outer ear
More than 80% of patients with TS have ear malformations, including low set ears, elongated ears, cup-shaped ears and thick ear lobes.

Middle Ear
Otitis media is extremely common in girls with TS and may progress to mastoiditis and/or cholesteatoma formation. It occurs particularly between 1 and 6 yr of age, with a maximum incidence (>60%) at 3 yr of age. The cause is still unknown, but growth retardation of the temporal bone may be important. Aggressive treatment of otitis media is appropriate, and insertion of ventilation tubes should be considered. Careful follow-up is important. Patients with chronic middle ear problems should be operated on without delay to prevent sequelae. Short girls with extensive otitis media problems should be referred to an endocrinologist if TS has not previously been diagnosed.
Inner Ear
The majority (50–90%) of women with TS have sensorineural hearing loss, manifest by a sensorineural dip in the 1.5–2 kHz region, sensorineural high frequency loss, or all of these. The sensorineural dip can occur as early as 6 yr of age and occasionally leads to hearing impairment during childhood. The condition is progressive, however, and commonly leads to hearing problems in later life, which may have serious social consequences.
Management
Obtain a baseline audiologic evaluation at the time of diagnosis of Turner’s Syndrome and follow-up annually, preferably before heading back to school in the Fall. Heightened surveillance for middle ear problems, especially in childhood. Follow-up with ORL specialist for medical management and audiologist to monitor hearing. If a hearing loss is identified – hearing aids may be recommend dependent on the type and severity of the hearing loss. If patient is of school age, an FM system may also be appropriate in academic settings.Academic/Education Support for Speech and Language Intervention.
Tips for Healthy Ears and Hearing for All
Refraining from cotton swab use on yourself or child.
Hearing conservation to prevent noise induced hearing loss or additional hearing loss or additional hearing loss from noise exposure.
Ear plugs should be utilized in high noise environments.
Reducing the volume and limiting time listening to personal audio devices.
References
American Speech-Language-Hearing Association | ASHA. (2011, October 10). American Speech-Language-Hearing Association| ASHA. Retrieved July 21, 2014, from
Newborn Hearing Screening. (2013, March 29). . Retrieved July 7, 2014, from
EHDI Legistlation: Overview. (2014, January 10). . Retrieved July 2, 2014, from
Anthony, T. (2011, February 2010). Spotlight on Turner Syndrome. . Retrieved July 1, 2014, from
Serra, A , Cocuzza, S., Caruso, E., Mancuso, M., & Martia, I L, Audiological range in Turner Syndrome. International Journal of Pediatric Otorhinolaryngology, 67, 841-845
Marimoto, et al. Hearing Loss in Turner Syndrome. The Journal of Pediatrics. 691-701
Parkin, M., & Walker, P. Hearing Loss in Turner Syndrome. International Journal of Pediatric Otorhinolaryngology, 73, 243-247.
Olveira, C.S., Ribeiro, F.M., lago, R., & Alves C. Audiological Abnormalities in Patients with Turner Syndrome. American Journal of Audiology, 22, 226-232
Incidence of Hearing Loss with Turners Syndrome. (2014, February 2). . Retrieved July 1, 2014, from
Jung, J.H. (1989). Genetic syndromes in communication disorders. Boston: College-Hill Press.
Hearing Aids Assistance Programs:
http://sertoma.org/ways-to-help/hearing-aid-resources/
Part C Eligibility Considerations: For Infants and Toddlers Who are Deaf or Hard of Hearing - National Center for Hearing Assessment and Management 2012
View White Papers on Ears and Hearing
back to top


Ophthalmological evaluation should be part of the regular physical examination. These are some possible issues:
Strabismus can be either a disorder of the brain in coordinating the eyes, or of one or more of the relevant muscles' power or direction of motion.
Amblyopia, also known as lazy eye, is a disorder of the visual system that is characterized by a vision deficiency in an eye that is otherwise physically normal, or out of proportion to associated structural abnormalities of the eye. It has been estimated to affect 1–5% of the population.
Ptosis is a drooping or falling of the upper or lower eyelid.
back to top

Short Stature
Short stature affects at least 95% of all individuals with TS and is the most consistent readily recognizable clinical feature of TS. Short stature in TS is characterized by mild intrauterine growth retardation, slow growth during infancy, delayed onset of the childhood component of growth, and growth failure during childhood and adolescence without a pubertal growth spurt. This growth failure leads to a reduced final height, which is approximately 20 cm below the female average of the corresponding ethnic group. The average height left untreated is 4'8".
Final adult height for patients treated by growth hormone are greater in patients who:
- Initiate treatment at a young age.
- Are relatively tall at start of treatment.
- Are short in relation to their parents.
- Are treated with high doses of GH.
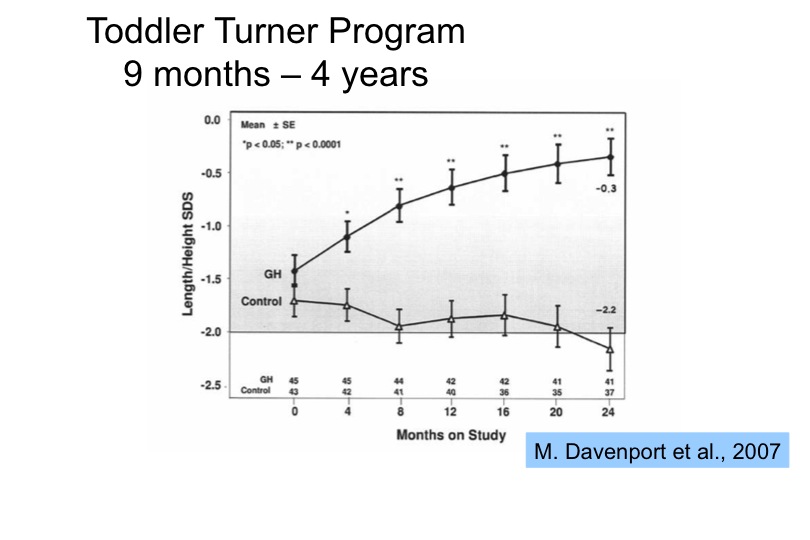
Growth hormone treatment is effective in most girls when started before the age of 9. The Toddler Study indicates an even more notable growth when treatment is initated very early in life during the toddler years.
Read more
Growth Hormones Assistance Programs are offered by a number of companies to assist patients and caregivers in obtaining information and suppport. Hormone Assistance Programs
back to top


Up to 40% of girls with Turner syndrome have hypertension, and when identified, it should be treated vigorously. Although in most cases hypertension is of unknown cause, a careful search for cardiovascular or renal causes should be made.
Blood pressure
Blood pressure is the force of your blood pushing against the walls of your arteries every time your heart beats. Your blood pressure is highest when your heart contracts, pumping the blood through your arteries. This is called systolic pressure. Your blood pressure is lowest when your heart is at rest, between beats. This is diastolic pressure.
Your blood pressure reading uses these two numbers, the systolic and diastolic pressures. Usually they are written one above or before the other:
119 (systolic)/79 (diastolic) or lower = normal blood pressure
120-139 for the top number, or 80-89 for the bottom number = pre-hypertension
140/90 or higher = high blood pressure
High blood pressure usually has no symptoms, except occasional headaches. It can cause serious problems such as stroke, heart failure, heart attack and kidney failure. You can control high blood pressure through healthy lifestyle habits and medication, if needed. A diagnosis of hypertension (a lasting medical condition where your blood pressure readings are consistently high) can only be made after a number of high blood pressure readings.
Blood pressure should be monitored at each physical examination. You may even have your blood pressure screened at your local pharmacy.
back to top


80 percent of women have increased liver parameters.
According to a recent paper, liver enzymes are elevated in patients and readily suppressed with hormone replacement therapy. A recent research paper, "Quantitive liver functions in Turner syndrome with and without hormone replacement therapy", 2007:
http://www.eje-online.org/content/156/6/679.long
back to top

Although most common in infants, lymphedema may occur or reoccur at any age, and may be associated with the initiation of therapy with GH or estrogen.

Presentation of newborn lymphedema
This article is a very brief overview of Turner Syndrome (TS). The information presented is based on the resources listed and the reader is encouraged to go to these sites to learn more about this condition.
What causes Turner Syndrome?
No known causes of TS have been found. There is nothing that parents do to cause or increase, the risk of TS in their daughters. Unfortunately there is also nothing they can do to prevent it. Based on the current knowledge, TS appears to be a random event that could happen to anyone [3].
What are the characteristics of Turner Syndrome?
Short stature and lack of ovarian development are two of the most common features of TS [3]. At the appropriate ages, these are treated with growth hormone and estrogen replacement therapy to stimulate a more normal growth pattern.
Other characteristics of TS vary greatly in their presence and their severity [4]. These include heart and kidney abnormalities, physical characteristics such as short neck, a low hairline and the back of the neck, and low-set ears.
Where does lymphedema come into this?
Lymphedema is present in about 70% of Turner Syndrome patients and the hands and feet are most commonly affected [4]. The form of lymphedema is the result of the underdevelopment of the lymphatic system before birth [1,p.14]. As the child matures, this swelling is managed using with the same treatment methods that are used to control other types of lymphedema.
How is Turner Syndrome diagnosed?
A prenatal ultrasound, such as the one shown here, may indicate that the fetus has a physical condition common to TS [1,p.8]. However the ultrasound alone does not provide a definite diagnosis.
What does the future look like for girls with Turner Syndrome?
With good medical and psychological care and the emotional support of friends and family, a girl with TS should look forward to a healthy and satisfying life. [1,p.34]
References and Resources
[1] New Turner Syndrome Guide for Families, which was written by Patricia Rieser, CFNP and Marsha Davenport, MD. This excellent guide is available, in both Spanish and English in a “ready to print” format.
[2] Turner Syndrome- US is the web site of the national Turner Syndrome organization. It contains information and helpful links.
[3] Living with Turner Syndrome- is an excellent informative site the fulfills the promise of its name by presenting helpful information on “Living with Turner Syndrome”
[4] Complications of Turner Syndrome is a part of the Turner Syndrome website that provides details on possible complications and includes information on TS clinical trials
What is Lymphedema?
- Lymphedema is abnormal swelling due to the presence of excess lymphatic fluid within the tissues. This swelling occurs when the lymphatic system malfunctions or is damaged and lymphatic fluid cannot drain as quickly as produced.
- Lymphedema affects an estimate 100 million men, women, and children around the world including at least 3 million Americans.
- Lymphedema occurs most commonly in the extremities (arms, or legs); however, it can also affect the trunk, breast, abdomen, neck, head, and or genitals.
- The fluid that causes the swelling of lymphedema is protein-rich and this makes the tissue easily susceptible to infections.
- Lymphedema is a chronic condition that can be treated but not cured. Early treatments can usually effectively control the condition.
- Without treatment, the lymphedema symptoms become progressively more serious. The seriousness of the condition is described as Stages of Lymphedema.
- The onset of lymphedema can be sudden, gradual, or delayed so that it appears years after the causative event.
The two principle types are PRIMARY lymphedema and SECONDARY lymphedema.
Primary Lymphedema
Primary Lymphedema is a hereditary abnormality of the lymphatic system that occurs in approximately one in six thousand people. Although the cause is not well understood, these abnormalities often include hypoplasia or hyperplasia. The swelling of primary lymphedema usually starts distally (at the far end of the limb) and spreads proximally (upward toward the body).
Primary congenital lymphedema is also known as Nonne- Milroy’s disease or Milroy’s disease it is either present at birth or develops within the first two years of life.
- Lymphedema praecox, also known as Meige disease, is primary lymphedema in which the symptoms begin at the time of puberty. Most cases of primary lymphedema present symptoms at this age and this condition affect mostly girls with symptoms in the lower extremities.
- Lymphedema tarda, is a primary lymphedema that occurs in adults and affects both males and females. The onset of symptoms in sudden, with no apparent cause, and can affect one or both of the lower extremities.
Secondary Lymphedema
Secondary Lymphedema is the result of a damaged or blocked lymphatic system. The swelling of secondary lymphedema usually begins near the body and spread towards the far end of the limb. Causes of secondary lymphedema include:
- Cancer treatment that involves the removal of the lymph node or their destruction due to radiation or chemotherapy. Shown here is secondary lymphedema following cancer treatment.
- Scars due to burns radiation treatment, or other damage to large areas of the skin.
- Trauma including all types of accidents, injuries, and surgery that damage to the lymphatic system.
- Those with chronic venous insufficiency can develop lymphedema as a secondary condition.
- Those who are obese can develop lymphedema as a secondary condition.
READ MORE ON LYMPHEDEMA DIAGNOSIS AND MANAGEMENT Read more...
Lymphatic Education & Research Network
www.lymphaticnetwork.org
Registry & Tissue Bank
https://lernregistry.stanford.edu/
Find Mismatched Shoes
https://search.oddshoefinder.com/
http://www.clarks.co.uk/helpandinfo/storesinstoreservices
http://oddshoefinder.com/oddshoesblog/faq/#whyfeet
http://www.abilityhacker.com/where-to-buy-shoes-when-your-feet-are-two-different-sizes/
http://www.oddshoe.org/index.php
http://www.ehow.com/facts_6883977_buy-shoes-feet-different-size.html
http://www.oddshoefinder.com/faq#whyfeet
Supplies
back to top
back to top

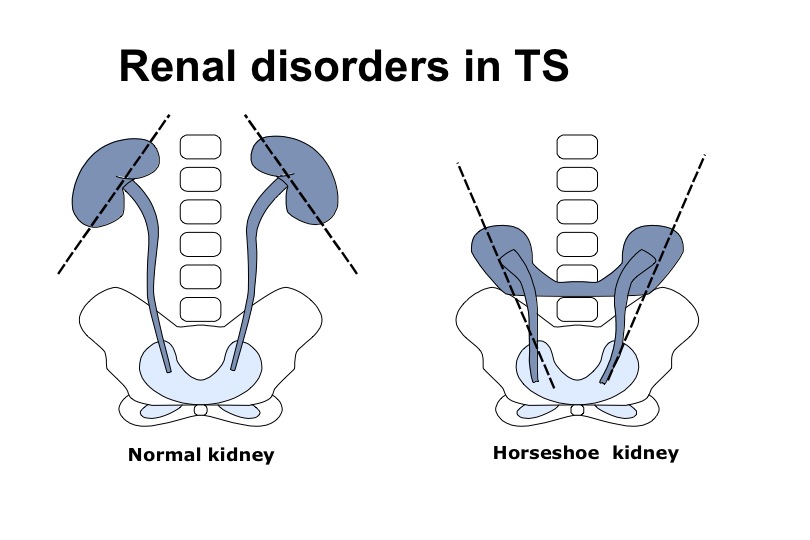
Urinary Tract Abnormalities
Approximately one third of patients with Turner syndrome have a structural malformation. Rotational abnormalities and double collecting systems, or abnormal vascular supply are found most frequently. Although many of these abnormalities do not have clinical significance, some may result in an increased risk of hypertension, urinary tract infections, or hydronephrosis. Therefore, all individuals with TS should have a renal ultrasound study performed at the time of diagnosis. If abnormalities are detected, further evaluations should be performed, and the appropriate therapy instituted. Additionally, in such individuals, ultrasound and urine cultures should be performed every 3–5 years.
back to top

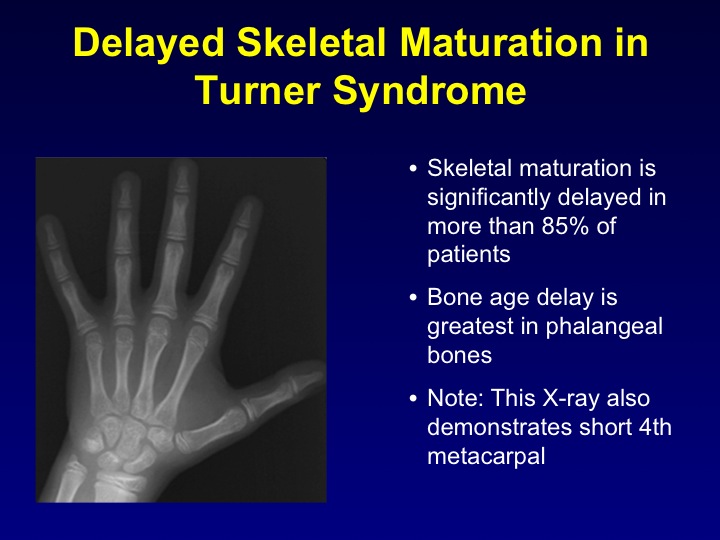
Orthopedic evaluation
Infants with TS have an increased risk of congenital hip dislocation, which may be associated with degenerative arthritis of the hips in older women. Approximately 10% of girls with TS develop scoliosis, most commonly during adolescence.
Characteristics:
Wide short neck, broad chest and square torso, outward turned arms, short metacarpal, and the cardinal indication short stature are commonly seen in Turner Syndrome. This photo is an example of Madeleung deformity Osteotomy of the Radius and Ulna for Madeleung deformity

Orthopedic Problems
Congenital developmental dysplasia of the hip occurs more frequently in girls with Turner syndrome than in the general population. This contributes to the development of arthritis of the hips in older individuals. Girls with Turner syndrome also have an increased risk of scoliosis, over curviture of the over-curvature of the thoracic vertebrae, or swayback an overexagerated curve in the lower spine.
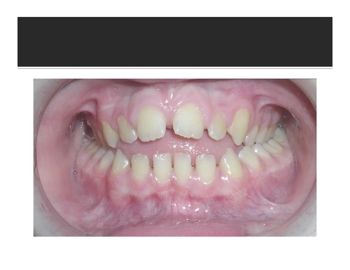
Orthodontic Issues
The small and retrognathic mandible may contribute to malocclusion and other dental abnormalities. An orthodontic examination should therefore be undertaken at 8–10 yr of age.
Craniofacial Anomalies
If craniofacial anomalies cause concern, consider plastic surgery for the neck, face, or ears before the child enters school or thereafter, as indicated. Some individuals with Turner syndrome have a tendency to form keloids, which must be taken into account when surgery is considered.
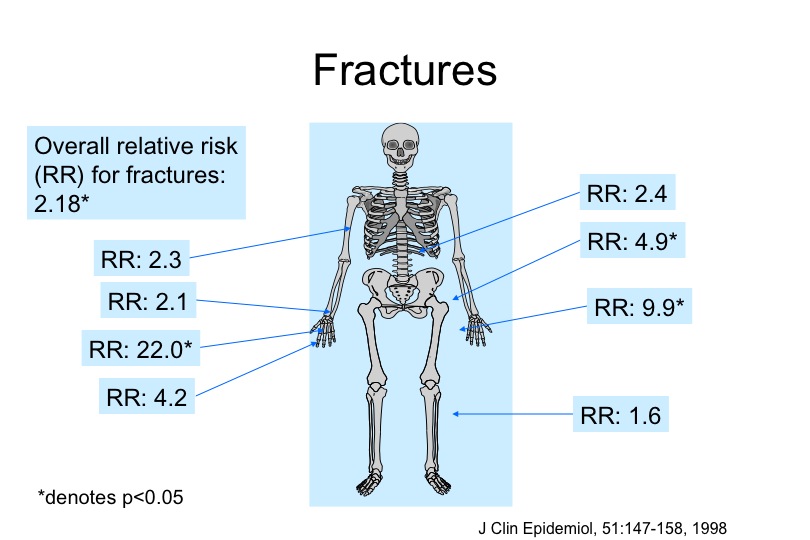
There is a high incidence of osteoporosis—meaning thin or weak bones—in women with Turner syndrome. Osteoporosis leads to loss of height, curvature of the spine and increased bone fractures.
The primary cause of osteoporosis in individuals with Turners appears to be inadequate circulating estrogen in the body. Turner women who have low levels of estrogen due to ovarian failure can take estrogen treatments, which will help prevent osteoporosis. It is possible that other factors contribute to the severity of osteoporosis in Turner syndrome. For example, there may be defects in bone structure or strength related to the loss of unknown X-chromosome genes. This is an area of major medical significance, which demands further study to help prevent osteoporosis and fractures in women with Turner syndrome.
What is osteoporosis?
Osteoporosis, or porous bone, is a disease in which there is a loss of bone mass and destruction of bone tissue. This process causes weakening of the bones and makes them more likely to break. The bones most often affected are the hips, spine, and wrists.
Who is affected by osteoporosis?
Osteoporosis affects over 10 million Americans, with women four times more likely to develop osteoporosis than men. Another 34 million have low bone mass and therefore have an increased risk for osteoporosis. Estrogen deficiency is one of the main causes of bone loss in women during and after menopause. Women may lose up to 20 percent of their bone mass in the five to seven years following menopause.
Other risk factors for osteoporosis:
Although the exact medical cause for osteoporosis is unknown, a number of factors contribute to osteoporosis, including the following:
- Aging
bones become less dense and weaker with age.
- Race -
Caucasian and Asian women are most at risk, although all races may develop the disease.
- Body weight -
Obesity is associated with a higher bone mass, therefore people who weigh less and have less muscle are more at risk for developing osteoporosis.
- Lifestyle factors:
The following lifestyle factors may increase a person's risk of osteoporosis:
- physical inactivity
- caffeine
- excessive alcohol use
- smoking
- dietary calcium and vitamin D deficiency
- Certain medications
- Family history of bone disease
What are the symptoms of osteoporosis?
Persons with osteoporosis may not develop any symptoms, or may have pain in their bones and muscles, particularly in their back. The symptoms of osteoporosis may resemble other bone disorders or medical problems. Always consult your physician for a diagnosis.
How osteoporosis is diagnosed:
In addition to a complete medical history and physical examination, diagnostic procedures for osteoporosis may include the following:
- Family medical history
- X-rays (skeletal) - a diagnostic test which uses invisible electromagnetic energy beams to produce images of internal tissues, bones, and organs onto film.
- Bone density test (Also called bone densitometry.) - measurement of the mass of bone in relation to its volume to determine the risk of developing osteoporosis.
- Blood tests (to measure serum calcium and potassium levels)
The effects of this disease can best be managed with early diagnosis and treatment.
Treatment for osteoporosis:
Specific treatment for osteoporosis will be determined by your physician based on:
• Your age, overall health, and medical history
• Extent of the disease
• Your tolerance for specific medications, procedures, or therapies
• Expectations for the course of the disease
• Your opinion or preference
The goals of managing osteoporosis are to decrease pain, prevent fractures, and minimize further bone loss. Some of the methods used to treat osteoporosis are also the methods to help prevent it from developing, including the following:
• Maintain an appropriate body weight.
• Increase walking and other weight-bearing exercises.
• Minimize caffeine and alcohol consumption.
• Stop smoking.
• Maintain an adequate intake of calcium through diet and supplements. Vitamin D is also necessary because it facilitates the absorption of calcium.
• Prevent falls in the elderly to prevent fractures (i.e., install hand railings, or assistive devices in the bathroom, shower, etc.).
• Consult your physician regarding a medication regimen.
For postmenopausal osteoporosis in women, the US Food and Drug Administration (FDA) has approved the following medications to maintain bone health:
• estrogen replacement therapy (ERT) and hormone replacement therapy (HRT)
ERT has proven to reduce bone loss, increase bone density, and reduce the risk of hip and spinal fractures in postmenopausal women. However, a woman considering ERT should consult her physician, as the recent study conducted by the National Heart, Lung, and Blood Institute of the National Institutes of Health (NIH) found health risks associated with this therapy.
• alendronate
This medication, from a group of medications called bisphosphonates, reduces bone loss, increases bone density, and reduces the risk of fractures.
• risedronate sodium (Actonel®)
This medication is also from the bisphosphonate family and has similar effects as alendronate.
• raloxifene (Evista®)
This medication is from a new group of medications called selective estrogen receptor modulators (SERMs) that help to prevent bone loss.
While this information is provided to be helpful, it is not meant to be medical advice. Consult your physician if you have any questions or concerns.
Source:
http://www.rwjuh.edu/rwjuh/healthlibrary/36900.aspx
Resources:
Turner syndrome and osteoporosis: mechanisms and prognosis.
http://www.ncbi.nlm.nih.gov/pubmed/9685448
Vitamin D in the New Millenium white paper
Vitamin D Synopsis, Everything You Need to Know, by Sunil Wimalawansa pdf
Isolated SHOX Deficiency Leads to Similar Bone Geometry white paper
Bone Health FAQ's (frequently asked questions)
back to top

Plastic Surgery
The risk of significant scarring and keloid formation in patients with Turner Syndrome is high. Elective surgery (e.g. for webbed neck or prominent ears) should be employed judiciously. This also applies to simple procedures, such as ear piercing.
Nail Dysplasia
Nail dysplasia is found in 70% of all patients primarily due to a lymphatic response. The nails may appear small, narrowed, upturned, or deeply inserted at an angle, and some patients may not have toenails.
back to top

Occupational Therapy
Occupational therapists are trained to assist people of all ages to perform the functional tasks that normally occupy their lives. The "occupations" of childhood are play, activities of daily living (feeding, toileting, dressing, grooming, mobility), learning and school performance; learning skills in order to become functional and independent adults.
Education and strategies to modify or compensate to improve function and abilities are taught to achieve the individuals highest level of independence and overall quality of life.
These skills include:
• Regulation of arousal level in order to attend
• Refinement of sensory processing and discrimination
• Continual refinement and development of motor skills(gross & fine)
• Development of communication skills
• Appropriate engagement/affect and social interactions
• Language and cognitive skills
• Age appropriate self care skills
• Developing a positive self concept
Some examples:
- Girl’s with Turner Syndrome usually walk late and have poor coordination. OT can address motor skills and coordination through gross motor activities, sensory activities and play to increase balance, coordination, motor planning, strengthening and endurance.
- Girl’s with Turner Syndrome often have trouble with executive processing, planning and flexibility. OT can help the client develop and utilize the skills to be able to accept change and increase flexibility and help the client to express concerns and frustrations in an appropriate manner.
- Girls with Turner Syndrome require more structure to socialize and to complete tasks, and experience increased difficulty in understanding and interpreting social cues. OT can focus on building and understanding social skills by modeling age appropriate interactions, providing lessons, and forming instructional social groups.
Speech
Girls with TS often have speech problems, speech therapist is recommended.
back to top

Between 10–30% of individuals with TS develop primary hypothyroidism, Hashimoto thyroiditis. Levels should be measured at the time of diagnosis and at intervals of 1–2 years thereafter.
Hashimoto’s thyroiditis (also called autoimmune or chronic lymphocytic thyroiditis) is the most common thyroid disease in the United States. It is an inherited condition that affects over 10 million Americans and is about seven times more common in women than in men.
Hashimoto’s thyroiditis is characterized by the production of immune cells and autoantibodies by the body’s immune system that can damage thyroid cells and compromise their ability to make thyroid hormone. Hypothyroidism occurs if the amount of thyroid hormone which can be produced is not enough for the body’s needs. The thyroid gland may also enlarge, forming a goiter.
Causes
Hashimoto’s thyroiditis results from a malfunction in the immune system. When working properly, the immune system is designed to protect the body against invaders such as bacteria, viruses and other foreign substances. The immune system of someone with Hashimoto’s thyroiditis mistakenly recognizes normal thyroid cells as foreign tissue, and it produces antibodies that may destroy these cells. Although various environmental factors have been studied, none have been positively proven to be the cause of Hashimoto’s thyroiditis.
Signs & Symptoms
Hashimoto’s thyroiditis may not cause symptoms for many years and may remain undiagnosed until an enlarged thyroid gland or abnormal blood tests are discovered as part of a routine examination. When symptoms do develop, they are either related to local pressure in the neck caused by the goiter itself or to the low levels of thyroid hormone.
The first sign of this disease may be painless swelling in the lower front of the neck. This enlargement may eventually become easily visible. It may be associated with an uncomfortable pressure sensation in the lower neck, and this pressure on surrounding structures may cause additional symptoms, including difficulty swallowing.
Although many of the symptoms associated with thyroid hormone deficiency occur commonly in patients without thyroid disease, patients with Hashimoto’s thyroiditis who develop hypothyroidism are more likely to experience the following:
- Fatigue
- Drowsiness
- Forgetfulness
- Difficulty with learning
- Dry, brittle hair and nails
- Dry, itchy skin
- Puffy face
- Constipation
- Sore muscles
- Weight gain
- Heavy menstrual flow
- Increased frequency of miscarriages
- Increased sensitivity to many medications
The thyroid enlargement and/or hypothyroidism caused by Hashimoto’s thyroiditis progresses in many patients, causing a slow worsening of symptoms. Therefore, patients should be recognized and adequately treated with thyroid hormone. Optimal treatment with thyroid hormone will eliminate any symptoms due to thyroid hormone deficiency, usually prevent further thyroid enlargement, and may sometimes cause shrinkage of an enlarged thyroid gland.
Diagnosis
A physician experienced in the diagnosis and treatment of thyroid disease can detect a goiter due to Hashimoto’s thyroiditis by performing a physical examination and can recognize hypothyroidism by identifying characteristic symptoms, finding typical physical signs and performing appropriate laboratory tests.
Tests
Antithyroid Antibodies-Testing for increased antithyroid antibodies provides the most specific laboratory evidence of Hashimoto’s thyroiditis, but the antibodies are not present in all cases.
TSH (Thyroid-Stimulating Hormone or Thyrotropin) Test – Increased TSH level in the blood is the most accurate indicator of hypothyroidism. TSH is produced by another gland, the pituitary, which is located behind the nose at the base of the brain. The level of TSH rises dramatically when the thyroid gland even slightly underproduces thyroid hormone. So, in patients with normal pituitary function, a normal level of TSH reliably excludes hypothyroidism.
Free thyroxine estimate - the active portion of all of the thyroxine circulating in the blood. A low level of free thyroxine is consistent with thyroid hormone deficiency. However, free thyroxine values in the “normal range” may actually represent thyroid hormone deficiency in a particular patient, since a high level of TSH stimulation may keep the free thyroxine levels “within normal limits” for many years.
Fine-needle aspiration of the thyroid - usually not necessary for most patients with Hashimoto’s thyroiditis, but a good way to diagnose difficult cases and a necessary procedure if a thyroid nodule is also present.
Treatment
For patients with thyroid enlargement (goiter) or hypothyroidism, thyroid hormone therapy is clearly needed, since proper dosage corrects any symptoms due to thyroid hormone deficiency and may decrease the goiter’s size. Treatment generally consists of taking a single daily tablet of levothyroxine. Older patients who may have underlying heart disease are usually started on a low dose and gradually increased, while younger, healthy patients can be started on full replacement doses at once.
While you may improve in many ways within a week, the full impact of thyroid medicine may take quite some time. For example, skin changes may take up to 3-6 months to resolve. Because of the generally permanent and often progressive nature of Hashimoto’s thyroiditis, it is usually necessary to treat it throughout one’s lifetime and to realize that dosage of medicine required may have to be adjusted from time to time.
Optimal adjustment of thyroid hormone dosage, guided by laboratory tests rather than symptoms alone, is critical, since the body is very sensitive to even small changes in thyroid hormone levels. Levothyroxine tablets come in 12 different strengths, and it is essential to take them in a consistent manner every day. If the dose is not adequate, the thyroid gland may continue to enlarge and symptoms of hypothyroidism will persist. This may be associated with increased serum cholesterol levels, possibly increasing the risk for atherosclerosis and heart disease. If the dose is too strong, it can cause symptoms of hyperthyroidism, creating excessive strain on the heart and an increased risk of developing osteoporosis.
- American Association of Clinical Endocrinologists
back to top
|